Neurodiversity information for parents and young people
[Amanda re title: what does 'antegrade' mean? Can we cut if we don’t need this word? Is it a word you will regularly use when you tell patients about this procedure? Google definition is ‘forward moving’ which does not help (!)]
About nephrostomy
Nephrostomy is a way of relieving the pressure on an obstructed kidney, without you having to have an operation.
We use images from an ultrasound scanner and an X ray machine to guide a thin plastic tube through your skin and into your kidney. This allows the buildup of urine in your kidney to drain to the outside.
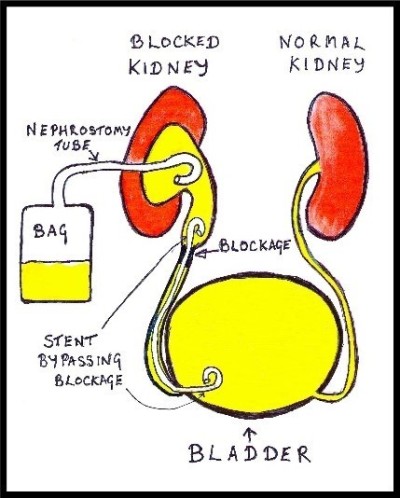
About ureteric stents
A ureteric stent is a thin plastic tube. We insert this stent inside your body, between your kidney and bladder.
Why you need a nephrostomy
Normally, urine flows from both kidneys to your bladder in thin tubes called ureters.
A test has shown that one (or both) of your ureters is blocked. This puts pressure on your kidney, preventing it from working properly and putting you at risk of infection.
Kidney stones and tumours are common causes of such blockages, and it is important that we relieve the pressure promptly. This will allow your kidney to recover function and drain any infection that may be developing.
Your doctors may already have tried to bypass the blockage from below, via a ‘cystoscopy’ (a small operation performed through your bladder). If this was unsuccessful, or if you were not a suitable candidate, then a nephrostomy is our standard approach.
Your doctor and your interventional radiologist feel this is the best initial treatment option for you.
They will discuss their recommendation with you and they will take your opinion into account. You will have the chance to ask questions. If, after discussion with your doctors, you do not want us to carry out the procedure, you can decide against it.
We will only go ahead with this procedure after you have given us your written consent.
Who performs the procedure and where it takes place
An interventional radiologist will perform your procedure. These doctors have special expertise in using X ray and scanning equipment and in interpreting the images produced. They use these images on screen to guide the procedure.
We will perform the procedure in the Interventional Radiology Unit, part of the Kingston Hospital Radiology Department.
Preparing for your procedure
Most patients having a nephrostomy procedure will already be in hospital, and will have had a previous scan showing obstruction of one or both kidneys.
To prepare for the procedure, do the following.
- You can take sips of water up to 2 hours before the procedure.
- You can take your normal medicines up until the procedure.
When you receive your appointment letter, tell the Interventional Radiology Unit if you have previously had allergies to foods, medicines or intravenous contrast medium (the dye used for kidney X rays and CT scans).When you receive your appointment letter, tell the Interventional Radiology Unit if you have been on blood thinning tablets such as warfarin, aspirin or clopidogrel.[Amanda: Can we cut these two bullets, or add a separate section for outpatient cases and put them there – as we have done with eg percutaneous fluid drainage?].- We may give you some pre-procedural painkillers and antibiotics if you need them.
When you arrive in the department, you will meet the team, including your nurse, interventional radiologist and radiographer. The radiographer operates the imaging equipment and is responsible for the images we take.
- We will ask you to lie on the X ray table, on your tummy but facing slightly to one side.
- We will already have inserted an intravenous cannula (a small, flexible tube inserted through a vein) prior to the procedure. This allows us to give you antibiotics, painkillers or sedation directly into the blood.
- We will wrap a cuff around your arm to monitor your blood pressure, and place a clip on your finger to measure your pulse and breathing.
- The doctor performing the procedure will choose the most appropriate point on your skin and will then clean this area with antiseptic and anaesthetise it with an injection. They will insert a fine needle through this numb area, into the kidney using the pictures from the scanner and X ray machine.
- Using a guidewire, they will exchange the needle for a plastic tube through which the build-up of urine in the kidney will drain to the outside.
- We will connect the tube to a bag, secure it with some stitches and cover it with dressings.
- Once we have successfully inserted the nephrostomy tube, it will relieve the pressure in your kidney and urine will start to drain into the external bag.
- This diverts the buildup of urine to the outside and leaves you with a plastic tube protruding from your skin. This is not a long-term solution, so the next step is often to insert a second tube called a ureteric stent.
Stent insertion
- This stent bypasses the original blockage and allows us to remove the external drainage tube. Usually, we perform this stent insertion as a separate procedure 48 hours after the initial drainage.
- If your nephrostomy insertion is straightforward and circumstances are favourable, we may insert the stent at the same time.
- We introduce the stent through the same route as the nephrostomy, so there is no need to create a new hole in your skin.
Pain
We give you pain killers and an injection of local anaesthetic to make sure your skin and deeper tissues go numb and the procedure is comfortable.
Everyone experiences pain differently and some people will find the procedure painful. If you feel pain, the nurse looking after you will be able to arrange stronger pain relief and sedation.
How long it takes
Every case is different, but you can expect to be in the X ray department for 1 to 2 hours. The amount of time depends on whether we insert a stent at the same time as the nephrostomy. Most of this time is spent in preparation for your procedure.
After the procedure
After the procedure, we will transfer you back to the ward [Amanda: what if they are outpatient? Radiology Recovery ward?].
It’s important that you remain comfortable and lie quietly in bed for a few hours until you have recovered. Back on the ward your nurses will monitor your pulse, blood pressure, breathing and temperature, to ensure you are recovering as expected.
We will give you an X ray (nephrostogram) approximately 48 hours after your stent insertion. This is to confirm that the stent is working properly and in a good position. If everything looks satisfactory, we can remove the external nephrostomy, leaving just the stent inside.
The stent does not specifically treat the underlying blockage; it only bypasses it.
It does allow time for us to further assess the cause of your blockage and plan the best treatment option for you.
Looking after your drainage tube
Your drainage tube is important for your recovery
Your nurse will check the bag regularly, to monitor how much fluid is draining and to prevent the bag becoming too heavy.
- Avoid pulling the tube out by accident while it remains in place.
- Avoid sudden movements.
- Always make sure that the attached bag can move freely with you.
- Avoid getting the tube twisted or pulled.
- Let your nurse know immediately if you think the tube has been pulled in any way.
Risks
Nephrostomy and stent insertions are safe procedures, and there are few serious risks or complications.
- Damage can occur to nearby bodily structures as we guide the tube into place.
- Bleeding can develop, although it is rare for this to cause a serious problem.
- If the fluid collection is infected, some infection can spread into your blood stream and give you a shivering attack, but we can usually treat this satisfactorily with antibiotics.
- On rare occasions we may not be able to place a stent correctly or, even if placed correctly, the stent may not work. If this happens you may require an operation.
If you have concerns or questions about this procedure, you can discuss these with your medical team and your interventional radiologist at any time.
Contact information
Interventional Radiology Unit
Interventional Radiology Unit Charge Nurse
Telephone:
Interventional Radiology Unit: 020 8934 6206
Interventional Radiology Unit Charge Nurse: 020 8934 2758