Neurodiversity information for parents and young people

If you read this information and decide you do not wish to go ahead, or want to consider alternatives, discuss this with your GP or hospital doctor. Do this as soon as possible before your appointment.
Key messages
1. Contact the nurse helpline now:
- if you are pregnant, or may be pregnant
- if you have a pacemaker
- if you have an implantable heart defibrillator
- if you take any medicine to help prevent clots, such as warfarin, rivaroxaban (Xarelto), apixaban (Eliquis), edoxaban (Lixiana) or dabigatran (Pradaxa)
- if you have a stoma.
2. Check the list of medicines to see if you need to change yours beforehand
Look at Medicines when having an endoscopy for details of which medicines must be stopped or changed beforehand.
3. Carefully read the bowel preparation instructions
Look at the instructions for bowel preparation we have also sent you. This must be started 3 to 7 days before the procedure. Your sigmoidoscopy may not go ahead if you have not completed the bowel preparation as instructed.
4. If you have diabetes, check the separate instructions
Look at Diabetes and having an endoscopy if you have diabetes.
5. Plan how you will get home
During the procedure, you may have medicines to relax you and relieve pain. If so, you must arrange to have a responsible adult to take you home and stay with you for 24 hours. During this time, you will not be able to, for example, drive, use the oven or kettle, go back to work or look after small children.
About a gastroscopy and sigmoidoscopy
Shared decision making and informed consent
Your healthcare team have suggested a gastroscopy and sigmoidoscopy. However, it is your decision to go ahead with the procedure or not. This document will give you information about the benefits and risks to help you make an informed decision.
Shared decision making happens when you decide on your treatment together with your healthcare team. Giving your ‘informed consent’’ means choosing to go ahead with the procedure having understood the benefits, risks, alternatives and what will happen if you decide not to have it. If you have any questions that this document does not answer, it is important to ask your healthcare team.
Once all your questions have been answered and you feel ready to go ahead with the procedure, you will be asked to sign the informed consent form. This is the final step in the decision-making process. However, you can still change your mind at any point.
Benefits
Your doctor is concerned that you may have a problem in your digestive system. They may have recommended a gastroscopy and sigmoidoscopy because you have been experiencing symptoms such as stomach pain, difficulty swallowing, bloating, diarrhoea and/or unexplained weight loss. Another reason might be that you do not have symptoms, but you are anaemic. This procedure is a good way of diagnosing most problems with your digestive system.
If the endoscopist (the person doing the procedures) finds a problem, they can perform biopsies (removing small pieces of tissue) to help make the diagnosis.
Sometimes a polyp (small growth) is the cause of the problem and the endoscopist may be able to remove it during the procedure.
Alternatives
Your healthcare team have suggested a gastroscopy and sigmoidoscopy as it a good way to help diagnosing most problems with your digestive system.
A colonoscopy is similar to a flexible sigmoidoscopy but the endoscopist looks all the way round your large bowel and the procedure has slightly higher risks. Other options include a CT colography (a CT scan of your large bowel).
If your doctor finds a problem, you may still need a gastroscopy or sigmoidoscopy to treat the problem or perform biopsies.
If you decide not to have the procedure or the procedure is delayed
Your healthcare team may not be able to confirm what is causing your symptoms, and they may get worse. If they do, you should speak to your healthcare team.
If you decide not to proceed, you should discuss this carefully with your healthcare team.
Before the procedure
Medicines
If you take warfarin, clopidogrel or other blood-thinning medication or are diabetic, let your healthcare team know at least 10 days before the procedure.
If you have diabetes, you will need special advice depending on the treatment you receive for your diabetes. Look at Diabetes and having an endoscopy with bowel preparation if you have diabetes.
If you take iron tablets, stop taking them at least 7 days before the procedure.
If you can, stop taking loperamide and codeine for 3 days before the procedure.
Look at Medicines when having an endoscopy for more details of which medicines must be stopped or changed beforehand.
Preparation
Look at the instructions for bowel preparation we have also sent you. This must be started 3 to 7 days before the procedure. Your sigmoidoscopy may not go ahead if you have not completed the bowel preparation as instructed.
You will need to follow a special diet and should be given information about this before the procedure. You will be given strong laxatives to take before the procedure. This is to make sure your large bowel is empty so the endoscopist can have a clear view. Laxatives can make you dehydrated, so drink plenty of fluids before the procedure. If you cannot drink fluids, have severe abdominal pain or continuously vomit, speak to your healthcare team. You may have a higher risk of dehydration or too much fluid if you are already dehydrated, older or are taking large doses of diuretics (water tablets) for heart or kidney disease.
Laxatives can affect how well your body absorbs medication. Do not take medication orally (by mouth) within one hour of taking the laxatives. If you are unsure of anything, speak to your healthcare team.
When you arrive

We will be happy to answer any questions when you come in. Please ask if you wish to discuss anything in private.
The healthcare team will carry out a number of checks to make sure you have the procedure you came in for. You can help by confirming your name and the procedure you are having with your healthcare team.
The healthcare team will ask you to sign the consent form once you have read this document and they have answered your questions. You will be asked to confirm your consent on the day of the procedure.
What the procedure involves
A gastroscopy and flexible sigmoidoscopy usually takes about 1 hour.
The endoscopist may offer you a sedative or painkiller to help you to relax. They will give it to you through a small needle in your arm or the back of your hand. You will be able to ask and answer questions but you will feel relaxed. You may not be aware of or remember the procedure. The healthcare team can give you more information about this.
In rare cases your endoscopist may perform the procedure with you asleep under a general anaesthetic. They can give you this through the small needle, or as a mixture of anaesthetic gas that you breathe through a tube which passes into your airways. This means you will be unaware of the procedure. There are complications associated with a general anaesthetic. The healthcare team can give you more information.
Once you have removed any false teeth or plates, they may spray your throat with some local anaesthetic and ask you to swallow it. This can taste unpleasant.
The endoscopist will ask you to lie on your left side and will place a plastic mouthpiece in your mouth. The healthcare team will monitor your oxygen levels and heart rate using a finger or toe clip. If you need oxygen, they will give it to you through a mask or small tube under your nostrils.
If you are awake during the procedure and at any time you want it to stop, let the endoscopist know. The endoscopist will end the procedure as soon as it is safe to do so.
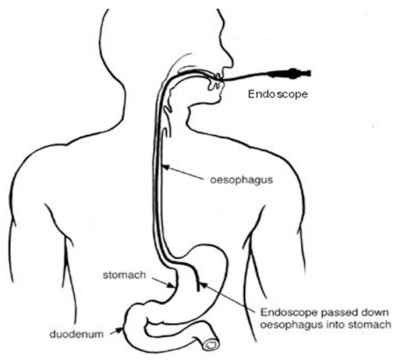
A gastroscopy involves placing a flexible telescope (endoscope) into the back of your throat. The endoscopist may ask you to swallow when the endoscope is in your throat. This will help the endoscope to pass easily into your oesophagus and down into your stomach. From here the endoscope will pass into your duodenum.
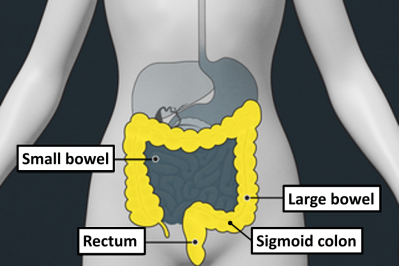
A flexible sigmoidoscopy involves placing a flexible telescope into your back passage and blowing some air into your large bowel to get a clear view. The endoscopist will usually examine up to the first 60cm of your large bowel.
The endoscopist will be able to look for problems such as inflammation, ulcers or polyps (small growths). They will be able to perform biopsies and take photographs to help make the diagnosis. If they find a polyp, it may be possible to remove it during the procedure.
Complications
The healthcare team are trained to reduce the risk of complications.
Any risk rates given are taken from studies of people who have had this procedure. Your healthcare team may be able to tell you if the risk of a complication is higher or lower for you.
Possible complications of this procedure are shown below from most to least likely. Some can be serious. Rarely, you may need to come back into hospital for more treatment, including surgery.
![]()
| Common More than 1 in 20 |
Pain during and after the procedure Procedure not completed
We may recommend a repeat procedure or an alternative investigation. |
| Less common Up to 1 in 20 |
Complications of sedation
Damage to teeth, lips or gums Missed abnormalities |
| Rare Up to 1 in 100 |
Hole in the bowel This is a serious complication but is very rare. Around 1 in 2000 cases result in a hole in the stomach or upper bowel, and around 1 in 3000 cases result in a hole in the lower bowel. The tear allows food contents to leak out and can cause severe infection and inflammation in the chest or abdomen. It may need a procedure or operation to repair it. Significant bleeding
|
After the procedure
After the procedure you will be transferred to the recovery area where you can rest.
If you were not given a sedative, you should be able to go home after a member of the healthcare team has spoken to you and decided you are ready. If you were given a sedative, you will usually recover in about 2 hour, but this depends on how much sedative you were given.
Do not eat or drink for at least the first hour after the procedure. Once you are able to swallow properly, you will be given a drink.
You may feel a bit bloated for a few hours, but this will pass.
The healthcare team will tell you what was found during the procedure and discuss with you any treatment or follow-up you need. Results from biopsies will not be available until a later date so the healthcare team will write to you, call you or ask you to come back to the clinic to give you the results.
Before you leave, you will be given a discharge advice sheet and a copy of your procedure report. The advice sheet will explain who to contact if you have any problems after your procedure. A copy of the report will be sent to your GP and doctor.

- if you go home the same day, a responsible adult should take you home in a car or taxi. They should stay with you for at least 24 hours unless your healthcare team tells you otherwise
- be near a telephone in case of an emergency
- do not drive, operate machinery or do any potentially dangerous activities (this includes cooking) for at least 24 hours and not until you have fully recovered feeling, movement and co-ordination
- do not sign legal documents or drink alcohol for at least 24 hours.
You should be able to return to work the next day unless you are told otherwise.
Once at home, if you get pain in your chest or abdomen, have difficulty breathing, significant or continued bleeding from your back passage, a high temperature, or you vomit, contact the endoscopy unit or your GP. In an emergency, call an ambulance or go immediately to your nearest emergency department.
Summary
A gastroscopy and flexible sigmoidoscopy is usually a safe and effective way of finding out if there is a problem with your digestive system. However, complications can happen. Being aware of them will help you make an informed decision about surgery. This will also help you and the healthcare team to identify and treat any problems early.
Contact us
Endoscopy nurses helpline:
020 8934 6614 (2pm to 4pm only)
We strongly advise you read this information carefully before calling us. The answers to your questions may already be covered.
Call for questions relating to your procedure, medicines, or preparation for your test, which is not included in this leaflet and needs to be answered before you attend your appointment.
Make sure you have your hospital number ready before calling together with your full name and date of birth. Have a pen and paper ready too in case you need to write down information.
To reschedule or cancel appointments
Endoscopy Bookings: 020 8934 2099 option 2 (9am to 5pm) or Email khn-tr.
Your appointment is valuable. If you need to change your appointment, give us as much notice as possible, preferably at least 10 days. This allows us to offer the appointment to another patient.
Please note, the booking team cannot answer questions relating to the procedure.